


1Infectious Diseases and Dermatology Unit, Hospital of Fréjus-Saint-Raphaël, 2Private Dermatology Office, Blausasc, 3The miner’s house clinic, Vence, and 4Private Dermatology Office, Enghien-les-Bains, France
Cutaneous larva migrans is a dermatitis, typically acquired in warm tropical or sub-tropical countries, caused by migration of the larvae of nematodes (hookworm; mainly Ancylostoma braziliense and, occasionally, A. caninum or Uncinaria stenocephala), which are parasitic on animals such as cats and dogs, into the patient’s skin. The larvae penetrate the skin after contact with infected soil and cause a typical creeping eruption. Patients with cutaneous larva migrans seen in Europe have usually acquired the disease following a stay in a tropical or sub-tropical area. How-ever, some cases of cutaneous larval migrans are acquired in Europe. We report here 5 autochthonous cases in France and give an overview of European autochthonous cases.
Key words: cutaneous larva migrans; France; Europe; Ancylostoma caninum.
Accepted May 9, 2019; E-published May 10, 2019
Acta Derm Venereol
Corr: Pascal Del Giudice, Infectious Diseases and Dermatology Unit, Hospital of Fréjus-Saint-Raphaël, 240 avenue saint Lambert, FR-83600 Fréjus, France. E-mail: del-giudice-p@chi-fsr.fr
Cutaneous larva migrans is a dermatitis acquired in warm tropical and sub-tropical countries caused by the skin migra-tion of larvae of animal nematodes. However, some patients may present a cutaneous larva migrans acquired locally in Europe. We report herein 5 autochthonous cases in France and give an overview of the European autochthonous cases published over a period of 25 years.
Cutaneous larva migrans (CLM) is typically acquired in warm tropical or sub-tropical countries (1–3). CLM is a dermatitis caused by migration of the larvae of nematodes (hookworm; mainly Ancylostoma braziliense and, occasionally, Ancylostoma caninum or Uncinaria stenocephala (1–3)), which are parasitic on animals such as cats and dogs, into the patient’s skin. The larvae penetrate the skin after contact with infected soil and cause a typical creeping eruption (1–3). According to Caumes & Danis (4) a creeping eruption is defined by a linear or serpiginous cutaneous track that is slightly elevated, erythematous and mobile. The larvae cannot penetrate the skin basal membrane, therefore they progress within the epidermis, and the disease is self-limiting (3). This eruption must be distinguished from other non-creeping linear or serpiginous dermatoses, such as superficial thrombophlebitis, Mondor’s disease, lichen striatus and other lichenoid eruptions of this type, phytophotodermatitis, and zoster. Other creeping eruptions caused by parasites include larva currens, caused by Strongysloides stercoralis, gnathostomiasis, and Pelodera strongyloides, but the clinical presentation of these eruptions differs from typical CLM in most cases and these parasites are not endemic in France. Topical ivermectin is the most recent proposed therapeutic option (5, 6).
Patients with CLM in Europe have typically acquired the disease after a stay in a tropical or sub-tropical area. Europe, even Southern Europe, is not an endemic area for CLM; nevertheless, a few cases of autochthonous (locally acquired) CLM have been reported in Europe. We report here 5 autochthonous cases in France and give an overview of the European autochthonous cases of the last 25 years.
A 50-year-old woman was referred with a pruritic skin lesion on her wrist on 15 July 2011. She had a pruritic serpiginous linear cutaneous track on the right wrist that had evolved from a palmar papule within a few days (Fig. 1a). The physical examination was otherwise unremarkable. She had visited a sandy beach in Saint-Raphael (Var department) in the South of France on 2 and 9 July 2011 and had lain on towels placed directly on the sand. She was accompanied by her husband and daughter who were free of lesions. She had not travelled outside France for the last 2 years. She preferred not to receive treatment and to wait. On the 19 July 2011, the lesion disappeared spontaneously.
Fig. 1. Clinical presentation of cutaneous larva migrans (CLM) in patients 1–5 (a–e) (patient 1 was diagnosed by authors PDG and SH, patient 2 by PDG and TH, patient 3 by TH, patient 4 by FV and patient 5 by CM).
A 21-year-old man was seen on 21 August 2013 for a pruritic skin rash on the buttock lasting for 10 days. He used to swim in the river near Draguignan (Var department) and to lie on the bank of the river. The patient had been treated with fusidic acid cream with no effect. Clinical examination revealed an erythematous, crusted plaque-like eczema. Close examination of the plaque revealed serpiginous tracks typical of CLM (Fig. 1b). The patient was treated successfully with a single oral dose of 200 μg/kg ivermectin and clobetasol cream.
A 30-year-old man presented on 7 August 2015 with a serpiginous pruritic track on his back (Fig. 1c) after lying on a sandy beach at Sainte-Maxime (Var department). He had not travelled outside France within the past year. He did not recall when the lesion had first occurred. He was treated successfully with a single oral dose of 200 μg/kg ivermectin.
A previously healthy, 12-month-old boy presented on 17 June 2017 with a serpiginous skin track located on the buttock (Fig. 1d). The family had spent the weekend on the border of an artificial lake in the area of Oraison (Alpe-de-Haute-Provence department) on 11 June 2017. The family had not travelled within the previous 2 years. The diagnosis of CLM was clinically made, and the patient was treated successfully with a single oral dose of 200 μg/kg ivermectin.
A 60-year-old man living near Paris presented in September 2017 with pruritic serpiginous tracks on his back (Fig. 1e). He had not travelled outside France during the previous 2 years. The clinical diagnosis was consistent with CLM. He was treated successfully with a single oral dose of 200 μg/kg ivermectin.
We reviewed all autochthonous CLM reported in France and Europe over the last 25 years (1994–2018) (PubMed search, key words: “larva migrans”, “Europe”, and related references found in articles). A total of 55 cases were found: 15 from Spain (7–161), 13 from France, including ours (17–222), 9 from England/UK (23–30), 8 from Italy (31–33), 7 from Germany (34–37), 2 from Serbia (38), and 1 patient for whom it was not possible to determine whether they were was from Spain or Portugal (39). The geographical distribution of the cases in France and Europe is shown in Figs 2 and 3. The number of patients reported each year as listed in the published articles is shown in the histogram in Fig. 4.
Fig. 2. Map showing the number of autochthonous cutaneous larva migrans (CLM) case reports in each country in Europe (cases from Ireland and the UK are grouped together). Only the patient from reference 32 was not included on the map, since it was not possible to determine whether he was infected in Spain or Portugal. The map was created using the online LandsatLook Viewer (https://landsatlook.usgs.gov/).
Fig. 3. Map showing geographical origins of autochthonous cutaneous larva migrans (CLM) case reports in France. The map was created using the online LandsatLook Viewer (https://landsatlook.usgs.gov/).
Fig. 4. Histogram showing the number of autochthonous cutaneous larva migrans (CLM) patients reported in Europe, based on year of publication.
We report here 5 additional cases of autochthonous CLM in France and the first (3 patients) cases from the Mediterranean coast of France. The French Mediterranean border is characterized by more than 500 km of Mediterranean coastline with many sandy beaches, rivers and lakes. This area has temperate springs and hot summers. Millions of tourists visit each summer to enjoy the Languedoc-Roussillon, Provence and Riviera. In addition to these cases from southern France, other cases were from parts of the country such as the Brittany or Paris areas in the northern part of France, showing that autochthonous CLM is not restricted to the southern and warmest areas of the country. Autochthonous CLM had been reported previously in the early 20th century by Brocq in 1907 (40) and Darier in 1928 (41).
In Europe and France, CLM is usually an imported parasitic skin disease from tropical and overseas countries, but the number of autochthonous cases reported in the last 25 years shows that CLM is, in rare circumstances, a locally acquired disease in northern countries, such as Germany, the UK, or northern France. These observations may change our view of CLM as being typical of tropical diseases and exclusive to the tropics. One question raised by reports of autochthonous CLM in Europe is whether this increase can be ascribed to global warming; however, given the low number of cases reported yearly, it is not currently possible to give a definitive response. An incidence survey is indicated.
The authors thank Romain Blaizot for providing assistance with the bibliography, and Dr Cécile Delbarre (Villeneuve, France) for referring a patient.


 Click to show fullsize
Click to show fullsize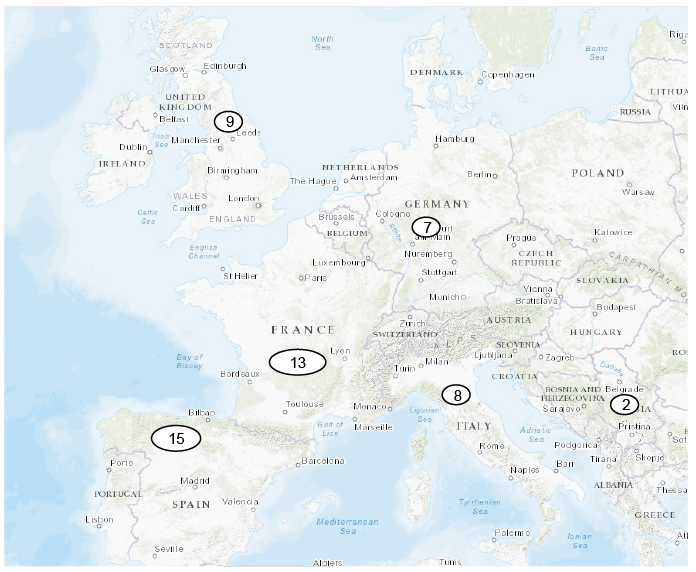 Click to show fullsize
Click to show fullsize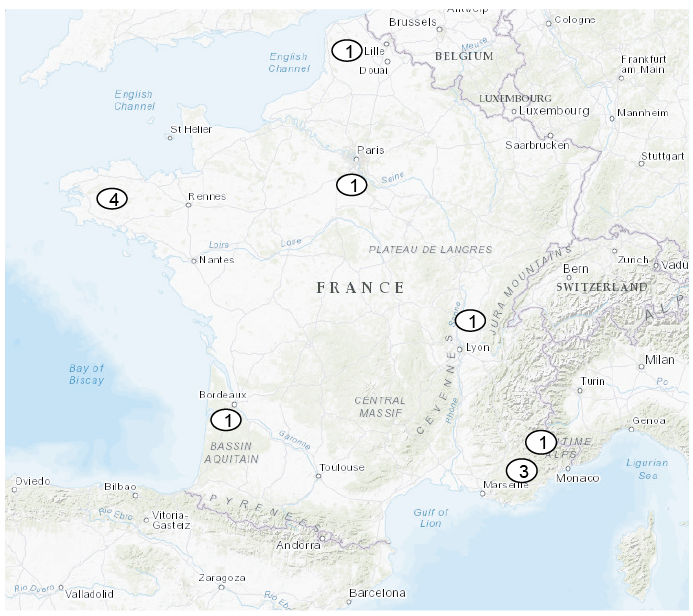 Click to show fullsize
Click to show fullsize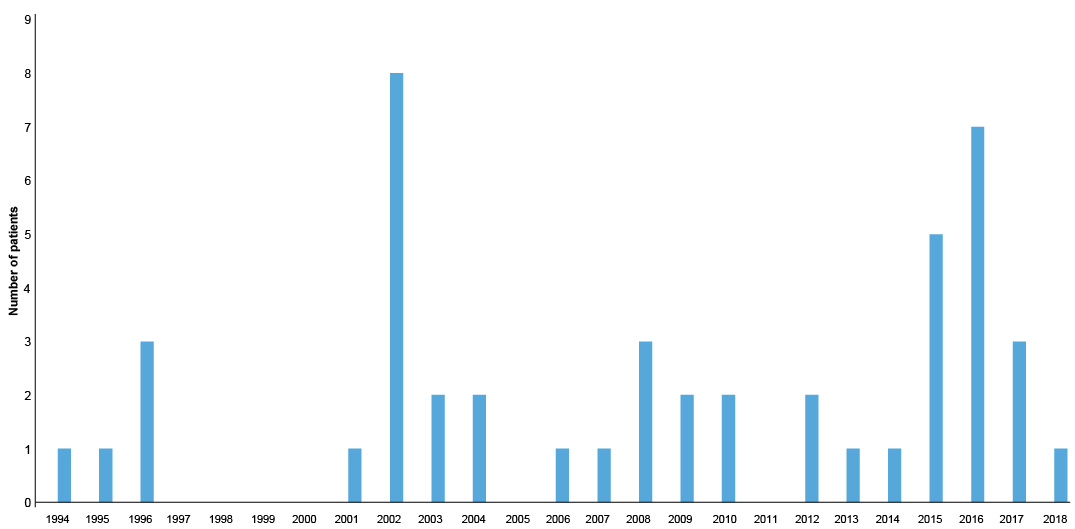 Click to show fullsize
Click to show fullsize